
Multi-Cancer Early Detection Tests: Misleading in Both Directions
A positive result often is a false alarm. A negative result is not a clean bill of health. The math explains why.


There is a particular kind of medical wishful thinking that is almost impossible to argue against in the exam room. A patient comes in having read about a new blood test that screens for fifty different cancers at once. Her neighbor had it done, and it identified pancreatic cancer before she had any symptoms or lab findings. Her brother-in-law had it done, got a clean result, and feels relieved. She wants it. The logic is just common sense, right? More testing means earlier detection means earlier treatment means longer life. What kind of doctor argues against that? Doctors like me, who have done the math.
Multi-cancer early detection (MCED) tests are becoming very popular: CancerGuard (Exact Sciences) and Galleri (GRAIL) are the most prominent. They detect fragments of tumor-derived DNA in the bloodstream using DNA methylation patterns (biochemical modifications) and other tumor-associated signals that differ between cancer and normal cells. They are being marketed directly to consumers and ordered by physicians despite lacking FDA approval, guideline endorsement, or a randomized controlled trial demonstrating that they reduce cancer mortality (1, 2). The intuition driving their adoption is understandable, but the mathematics underlying their performance in asymptomatic screening populations argues for considerable caution in both directions.
When the Test Is Positive
The leading MCED tests report specificity around 99.5%, meaning that among people who truly do not have cancer, the test correctly returns a negative result 99.5% of the time. That number sounds extraordinary, but in the context of population-level cancer screening, it’s actually pretty weak.
Why? Because the prevalence of asymptomatic cancer is low. In an asymptomatic screening population of people around age 50, the prevalence of any cancer detectable by an MCED test is ~0.5%, which means that only five people per thousand actually have cancer. The other 995 do not. A test with 99.5% specificity correctly identifies roughly 994 of those 995 cancer-free individuals as negative, but falsely flags ~5 as positive. With a sensitivity (the percent of people with cancer who the test identifies) around 50% (which is a reasonable aggregate figure across cancer types and stages), the test detects about 2 or 3 of the 5 true cancers. Among the 7 or 8 positive results generated, 5 are false positives. The positive predictive value (PPV), meaning the probability that a positive result reflects a real cancer, is only 30-40%.
The table below shows how PPV shifts with prevalence, holding test performance constant:
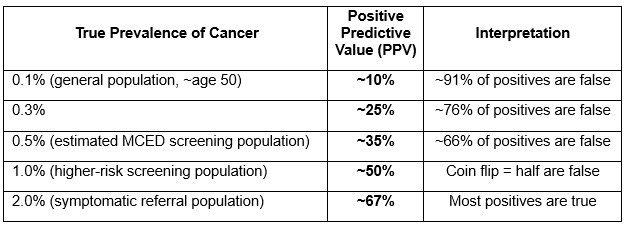
The test has not changed across any row of this table. Its sensitivity and specificity are fixed properties of the test and how it performs. What changes is the population: as prevalence falls, the enormous denominator of cancer-free individuals generates false positives that overwhelm the small numerator of true cancers. This is the Bayesian relationship between specificity and PPV, and it is inescapable. It’s math and it’s true, like water is wet and 1+1 = 2.
And it was shown to be true in a study of real people. In the PATHFINDER study, a prospective evaluation in an asymptomatic screening population (all of whom were over 50 and whose average age was 63 years), only 92 of 6,621 participants (1.4% screen positive rate) had a positive result, and only 35 were confirmed to have cancer (0.5% prevalence, leading to a PPV of 38% (3). Nearly half the signal-positive participants underwent biopsy or surgery (3). The math predicted what happened almost exactly.
There is an additional wrinkle: when a positive MCED result is followed by a PET-CT that reveals nothing, it remains genuinely unclear whether the patient is cancer-free or has a tumor too small to localize (4), which means the patient is left with uncertainty and worry - plus they are out a lot of money and have received additional radiation exposure and needle sticks.
But Even True Positives Are Not Simple
Suppose the test finds a real cancer. Our intuition says: good, we caught it early, now we can treat it. But there are at least three reasons this logic does not follow as reliably as it seems.
The first is stage distribution. MCED tests are better at detecting advanced disease than early disease. In the PATHFINDER study, less than half of the MCED-detected cancers were stage I or II, compared with nearly 3/4 detected by usual care (3). In a large real-world series of more than 100,000 Galleri tests, only 28% of signal-detected cancers were stage I or II, but nearly half were stage IV (5). Sensitivity for stage I disease in the CCGA validation cohort was approximately 17%, compared with roughly 90% for stage IV (6). A test that preferentially detects cancers that already are advanced has inverted the rationale for screening.
A test that preferentially detects cancers that already are advanced has inverted the rationale for screening.
The second is lead-time bias. Even when an MCED test detects a genuinely early-stage cancer, earlier detection does not automatically translate into longer survival; it can simply move the clock forward without changing when, or whether, the patient dies of that cancer (7).
The third is tumor biology: not all cancers that shed detectable ctDNA are cancers that will kill the patient on a relevant timescale. Some are slow-growing with natural histories measured in decades, so detecting them earlier does not extend life, but it does extend the period of knowing you have cancer, which can be its own harm. At the other extreme, the cancers where early detection might matter most, such as pancreatic, ovarian, and small-cell lung cancer, either are detected too late by MCED tests given the tests’ low stage I sensitivity, or have biology so aggressive that even a genuine stage shift does not reliably change outcomes. The cancers most amenable to early-detection benefit tend to be the ones already captured by existing single-cancer screening programs.
When the Test Is Negative
So what does all of this mean for the neighbor who got a clean result and feels reassured? Not so much.
With an aggregate sensitivity ~50%, a negative MCED result misses roughly half of the cancers present in the tested population. For stage I cancers, where detection might actually change outcomes (see previous section), the sensitivity falls to ~17%, meaning the test misses more than four out of five early-stage cancers. Although the negative predictive value (NPV, the probability that a person with a negative test truly does not have cancer) is high in absolute terms at ~99.75%, the probability of not having cancer before the test already was 99.5% in this population, so the test adds only ~0.25 percentage points of reassurance.
The practical implication is that a negative MCED result provides no justification for deferring established screening programs with demonstrated mortality benefit, such as colonoscopy, mammography, or low-dose CT for lung cancer in eligible smokers. Feeling relieved about a negative test is understandable, but it is a misreading of what the test result means.
The Evidence Still Has to Catch Up
No randomized trial has demonstrated that any MCED test reduces cancer mortality (1, 2). Although “lack of proof is not proof of lack,” the onus of proof is on the new test, and the math of screening in an asymptomatic population is not great. An independent model of the NHS-Galleri trial, the first RCT designed to test MCED screening with a stage-based primary endpoint, estimated a 6-9% reduction in 5-year cancer mortality under favorable assumptions (8), but models are hypotheses, not evidence. Indeed, the NHS-Galleri trial of nearly 143,000 UK participants aged 50–77 years recently reported results: it failed to meet its primary endpoint of reducing stage III–IV cancer diagnoses among 12 prespecified cancers in the screening arm, though a reduction in stage IV diagnoses was observed as a prespecified secondary endpoint (9,10).
As of today, the FDA has not approved any MCED test for population screening. Ordering an MCED test in an asymptomatic screening population means accepting an ~2/3 false-positive rate on positive results, low sensitivity for early-stage disease, no demonstrated mortality benefit, and the risk that a negative test result will be misinterpreted as reassurance it never was designed to provide.
As physicians, we are admonished not to practice anecdotal medicine. But to patients all that matters is what happens to them (or to their family member or friend) and the meaning they assign to it. The neighbor who caught an early pancreatic carcinoma: that is the expected outcome for ~1/3 of positive results in a screening population. It is good, but it is not clear that it ultimately helped, though I hope it did. The brother-in-law with the clean result who feels great should still get his colonoscopy. Both stories are real, but neither tells you what you need to know. The math does.
References
1. Kahwati LC, Avenarius M, Brouwer L, et al. Multicancer Detection Tests for Screening: A Systematic Review. Ann Intern Med 2025. doi:10.7326/ANNALS-25-01877.
2. Hoffman RM, Wolf AMD, Raoof S, et al. Multicancer Early Detection Testing: Guidance for Primary Care Discussions With Patients. Cancer 2025;131:e35823.
3. Prajapati H, Mody M, Kakadiya J, et al. Potential and pragmatism: Clinical and public health implications of multi-cancer early detection (MCED) screening via cfDNA in asymptomatic adults. J Clin Oncol 2026;44(Suppl 16):e22570.
4. Carr DJ, Welch HG. Assessing the Clinical Utility of Liquid Biopsies Across 5 Potential Indications From Therapy Selection to Population Screening. JAMA Intern Med 2023;183:1144–1151.
5. Matrana M, Shukla V, Kingsbury D, et al. Real-World Data and Clinical Experience From Over 100,000 Multi-Cancer Early Detection Tests. Nat Commun 2025;16:9625.
6. Klein EA, Richards D, Cohn A, et al. Clinical Validation of a Targeted Methylation-Based Multi-Cancer Early Detection Test. Ann Oncol 2021;32:1167–1177.
7. Welch HG, Dey T. Testing Whether Cancer Screening Saves Lives: Implications for Randomized Clinical Trials of Multicancer Screening. JAMA Intern Med 2023;183:1255–1258.
8. Gogebakan KC, Lange J, Owens L, et al. Clinical Significance of a Multicancer Screening Trial With Stage-Based End Points. JAMA Netw Open 2025;8:e2536247.
9. Galleri MCED Test Fails to Meet Primary Endpoint in Large Trial. Cancer Discov 2026 May 30:OF1. doi: 10.1158/2159-8290.CD-NW2026-0060.
10. The ASCO Post Staff. Annual Galleri Screening Reduced Stage IV Cancer Diagnoses but Missed Primary Endpoint in First Randomized MCED Trial. Posted: 6/2/2026; last updated: 6/4/2026. https://ascopost.com/news/june-2026/annual-galleri-screening-reduced-stage-iv-cancer-diagnoses-but-missed-primary-endpoint-in-first-randomized-mced-trial/
This is an excellent breakdown and translation of statistics to practice. Thank you! I can use this to explain the nuances to patients who ask about these tests though none so far have asked—perhaps because they are marketed directly to consumers.
Great post. I love how you laid out the numbers. I do find that many of my patients who are seeking more clarity on their longevity regarding cancer than what currently exists, are willing to pay, even if it’s only able to potentially change their outcome by a small margin or to provide a small margin of reassurance.
If this test were “free,”do you think it would be more widely adopted or isn’t the science there yet or would follow up testing create more medical debt than benefit?