
When Pictures Create Disease
How a Word on a Scan Becomes a Diagnosis and a Prescription

In my cardiology practice, one of the most common causes of iatrogenic disease - disease created by the medical system rather than by biology - is not a drug or a procedure, but a word embedded in a radiology report: “atherosclerosis.” It often begins with an X-ray or CT scan that detects arterial calcification and describes it using the pathological term “atherosclerosis” - rather than as an observation. That diagnosis takes on a life of its own, leading to a cascade of extra tests, medications, consultations, and patient anxiety that usually are unwarranted and sometimes are harmful.
The core problem is that an area of brightness is called “calcification” which then is diagnosed as “atherosclerosis,” or worse -“coronary artery disease” - without any meaningful patient context. Next, severity is assigned subjectively, without reference to age, cardiovascular disease (CVD) risk, or clinical context. And once the language of disease appears in a report, it changes how patients understand their health and how clinicians respond.
Here is an example of a recent chest CT report:
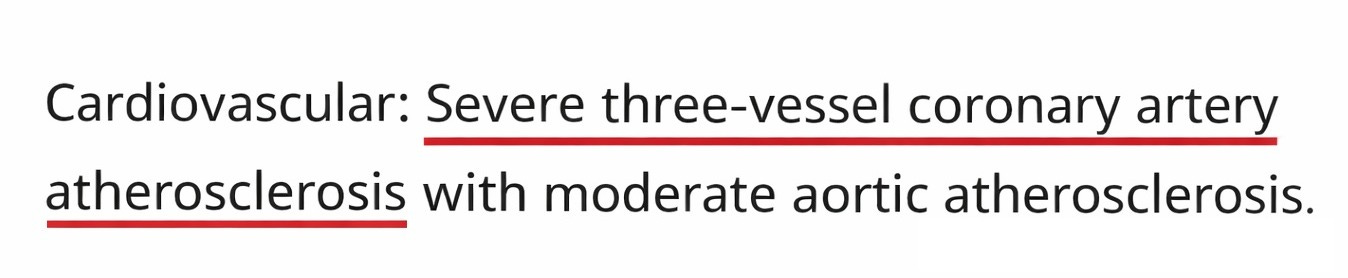
Three words do most of the work here: “severe,” “three-vessel,” and “atherosclerosis.” Each implies established, clinically significant disease. Although none of them, alone or together, establishes meaningful CVD risk without context, in practice they function as a diagnosis and drive what comes next.
This pattern of mislabeling brightness in a picture of an artery as a disease is remarkably consistent across organs and age groups. Coronary or aortic calcification regularly is described as “atherosclerosis.” Calcification of the cavernous or supraclinoid internal carotid arteries on a sinus CT is read as “vascular disease.” Bright lines on dental or neck X-rays become “carotid artery plaque,” and calcification on extremity films is labeled “peripheral arterial disease.” Different tissues, different imaging modalities, different arterial beds, and different specialists make the same conceptual error of converting an imaging observation into a tissue diagnosis. In each setting, the report’s label replaces clinical correlation.
What follows is a predictable cascade. Patients are started on aspirin and high-dose statins. They get a 12-lead electrocardiogram, a nuclear stress test is ordered, and they are referred to a cardiologist. Sometimes testing escalates to angiography. Radiation exposure increases. Incidental findings such as lung or liver nodules are discovered and they also can lead to further diagnostic cascades. Fear rises and the diagnosis of “coronary artery disease” appears on the chart, often permanently. All of this can occur before anyone has considered pretest probability, lifetime exposure to atherosclerotic CVD risk factors, or whether the imaging finding is even pathological in the first place. The label drives the workup rather than the biology or the symptoms. Interestingly, some patients develop symptoms after they are told they have “atherosclerosis,” often driven by hypervigilance and anxiety. The sequence is backwards: an incidental finding becomes a diagnosis, and the diagnosis generates the symptoms.
I want to be clear: everyone involved usually has good intentions. The radiologist believes that identifying “atherosclerosis” is clinically helpful. The primary care team feels obligated to evaluate it because it was named in the chart and the patient is worried. No one wants to miss something or face medical-legal risk. And it would be naïve not to acknowledge the financial incentives embedded in downstream testing.
The reasoning error is consistent: an imaging appearance is treated as a diagnosis, without consideration of pretest probability and cumulative exposure. The statistical name for this phenomenon is “base rate neglect.” When a finding is common in a given age group or population, labeling it as disease without considering its background prevalence distorts risk perception.
The CT report above came from a 65-year-old man with well-controlled lipids on a statin, no symptoms, and a calculated 10-year atherosclerotic CVD risk of 5%. Because the report noted “severe three-vessel coronary atherosclerosis,” he was put on aspirin and had his statin dose increased. A subsequent coronary CT angiogram showed no obstructive disease and his coronary artery calcium (CAC) score was near the population median for his age and sex. The imaging label implied high-risk disease, but the subsequent evaluation did not.
In a 22-year-old, arterial calcification is exceptionally unlikely to represent atherosclerosis; it may reflect developmental or hemodynamic changes at arterial branch points. In a 78-year-old, calcification is common and often expected. Although most calcium in older adults reflects atherosclerosis, not all arterial calcium is intimal plaque. Medial calcification occurs with diabetes mellitus, chronic kidney disease, hyperparathyroidism, and other disorders of calcium metabolism. Statin therapy is associated with increasing CAC as plaques stabilize and lipid content declines. Endurance exercise is associated with higher CAC scores as well. The point is that the biological meaning of calcification depends on the context. Calcium is a structural marker. It is not a direct measure of active atherogenesis, plaque instability, or short-term risk.
There are data to guide us. In a 2023 publication (1), my colleagues and I summarized the prevalence of detectable CAC on chest CTs in the Multi-Ethnic Study of Atherosclerosis. CAC prevalence exceeds 50% in some groups by the early 50s and approaches 90% by the early 70s, in others. When background prevalence approaches 50% or higher, the mere presence of calcium cannot be equated with pathological disease in the absence of clinical assessment.
Our current pattern of making diagnoses with acontextual pictures is a reversal of how medical diagnosis is supposed to work. When structural findings are detached from biology and base rates, we expand the denominator of illness without necessarily improving outcomes. This is the mechanism of overdiagnosis.
Overdiagnosis is expensive and anxiety-provoking, as patients are told that they have “severe” or “advanced” pathology based on subjective findings that are common and biologically heterogeneous. They live for weeks or months inside an unresolved diagnosis while cascades unfold. Over time, their identity shifts from “person” to “patient with heart disease,” often unnecessarily.
Some argue that improved quantification through artificial intelligence will replace subjective phrases such as “advanced for age” with numeric estimates. That may help, but quantification without context still risks framing calcification as disease rather than as one data point within a broader spectrum of CVD risk.
The recently published 2026 ACC/AHA dyslipidemia guidelines (2) address incidental CAC directly, and their recommendations deserve scrutiny in this context. The Class I recommendation that incidental CAC “should be considered” in decision-making about lipid-lowering therapy is reasonable; consideration is not treatment, and clinical context still can govern the response. However, the Class IIa recommendations go further by suggesting statin initiation based on the degree of incidental calcification, without reference to age, background prevalence, pretest probability, or whether the finding is even abnormal for the patient’s demographic. A 72-year-old with a CAC score that falls near the population median for his age and sex would meet the threshold for moderate-intensity statin therapy under these recommendations. That is precisely the pattern this post describes: a finding that is common and biologically heterogeneous is treated as a diagnosis, and the diagnosis generates the prescription. The guidelines use the word “incidental” but then treat the finding as if it were a disease in need of treatment.
Imaging findings should inform risk assessment, not replace it; it is critical that we avoid making diagnoses without the full clinical context.
Reference:
1. Tattersall MC, et al. Incidental Coronary Artery Calcium on Chest CT in Persons Without Known Atherosclerotic Cardiovascular Disease. JAMA Intern Med 2023;183:1269-1270. doi: 10.1001/jamainternmed.2023.3317.
2. Blumenthal RS, Morris PB, Gaudino M, et al. 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2026 Mar 13:S0735-1097(25)10254-4. doi: 10.1016/j.jacc.2025.11.016.
This is happening more and more. Rads are noting calcium everywhere (and often very loose with terminology as you noted). And it’s definitely generating work for a general cardiologist like me. And this is in a Canadian context where the medico legal implications of such incidental findings are perhaps less dire than in the US.
As with most finding, context matters.